Visual Pharmacology · Step-by-Step Mechanisms
Mechanism of Action Flowcharts
Drug mechanisms mapped from receptor to response — signal transduction cascades, second messengers, and clinical endpoints visualised in one place.
1 Flowchart
Autacoids & Antagonists
Signal Transduction
Autacoids & Antagonists
1 flowchart
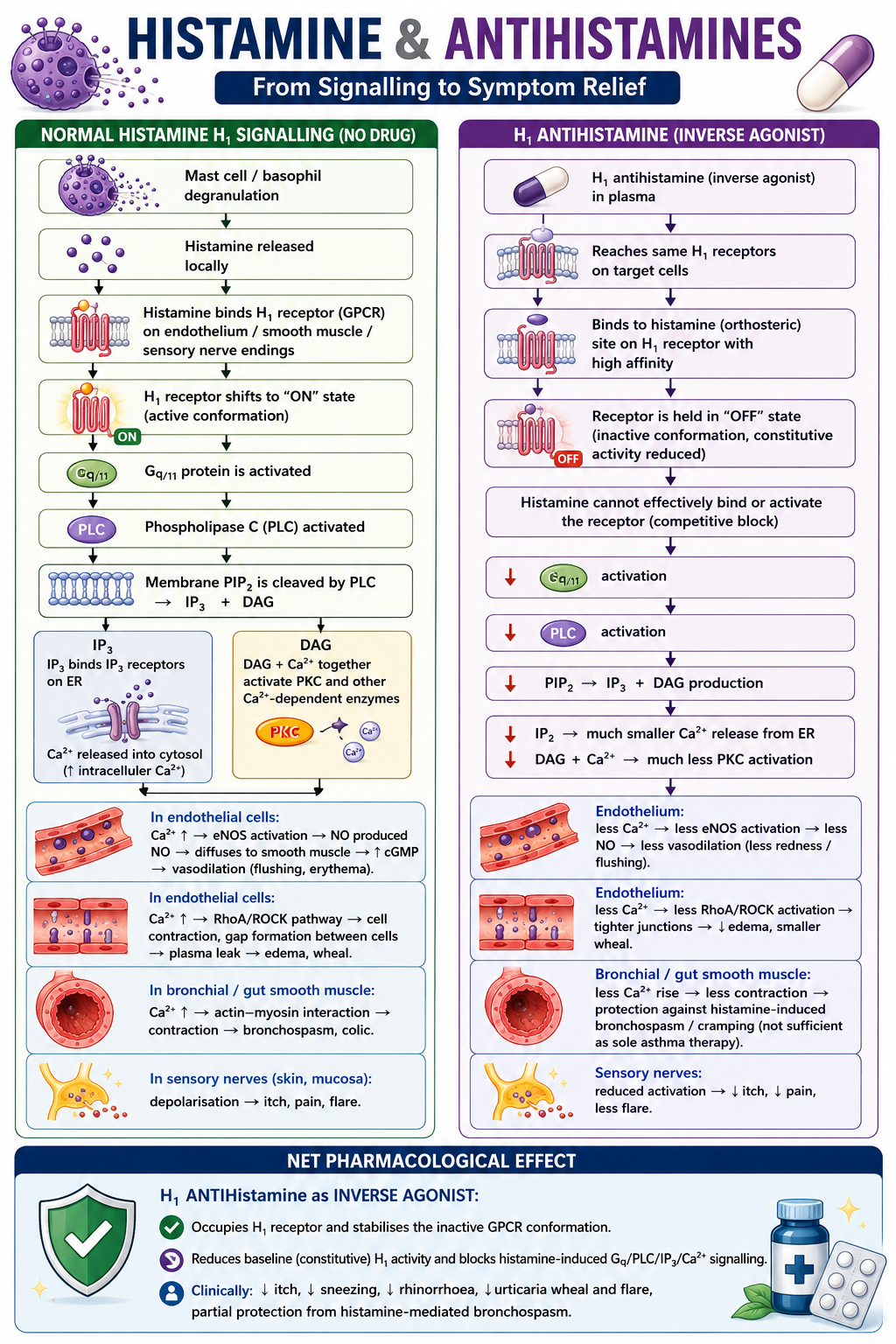
Histamine & Antihistamines — From Signalling to Symptom Relief
H₁ receptor signal transduction · Gq/PLC/IP₃/DAG/Ca²⁺ cascade · Inverse agonism explained
Autacoids
GPCRs
Gq/11 Pathway
Immune · Allergic
Key Pharmacological Points
H₁ receptor is constitutively active
H₁ is a GPCR with baseline (constitutive) activity even without histamine. Antihistamines are inverse agonists — they don't just block histamine; they stabilise the inactive receptor conformation and reduce baseline signalling below zero.
Gq/11 → PLC → IP₃ + DAG pathway
Histamine binding activates Gq/11 → PLC cleaves membrane PIP₂ into IP₃ (→ ER Ca²⁺ release) and DAG (→ PKC activation). Both branches drive the full allergic response: vasodilation, oedema, bronchoconstriction, itch.
Ca²⁺ is the master effector
In endothelial cells: Ca²⁺ → eNOS → NO → vasodilation (flushing/erythema). In vascular endothelium: Ca²⁺ → RhoA/ROCK → gap junction formation → plasma leak → oedema/wheal. In smooth muscle: Ca²⁺ → actin–myosin → contraction (bronchospasm, colic).
Inverse agonist ≠ competitive antagonist
A competitive antagonist blocks agonist binding but does not affect constitutive activity. An inverse agonist (like cetirizine, loratadine) additionally reduces the basal activity of the receptor below its unoccupied level — clinically important in chronic urticaria where spontaneous H₁ activation drives symptoms without exogenous histamine.
Why antihistamines don't stop all bronchoconstriction
Histamine-mediated bronchoconstriction involves H₁ on bronchial smooth muscle. Antihistamines reduce this but are not sufficient as sole asthma therapy because other mediators (leukotrienes, prostaglandins, PAF) maintain bronchospasm independently of H₁.
Clinical translation
↓ itch, sneezing, rhinorrhoea (H₁ on sensory nerves and nasal mucosa) · ↓ urticaria wheal and flare (vascular H₁ block) · partial bronchospasm protection · no effect on H₂-mediated gastric acid secretion (different receptor, different G-protein).